@mickebrown
Active 8 years, 6 months ago-

Micke Brown, BSN, RN posted a new activity comment 9 years, 3 months ago
Wonderful blog, Janice. I can smell the bread baking from here! My neighbor has a bread machine that she loves like you. She makes the best cinnamon rolls and they vanish quickly whenever she shares them with me. After all, lab studies have found that cinnamon may reduce inflammation, have antioxidant effects, and fight bacteria. The smell and…[Read more]
-
Micke Brown, BSN, RN wrote a new post 9 years, 3 months ago

Finally, Hollywood is talking about chronic pain. Or is it? Coming Soon—January 23, 2015, Cake will be showing in theaters. Jennifer Aniston is receiving accolades for her portrayal of a woman battling the […]
-
Micke Brown, BSN, RN posted a new activity comment 9 years, 4 months ago
Warning: Make sure you coat the “dough” with plenty of powdered sugar on BOTH sides before attempting to roll between the wax paper. If not, you will have one sticky mess on your hands! I learned the hard way but won in the end. WHEW!
-
Micke Brown, BSN, RN posted a new activity comment 9 years, 4 months ago
What a sweet story, Ruthie. I can imagine his face and your mother’s glee. Makes me warm all over during this bitter cold day in January.
-
Micke Brown, BSN, RN posted a new activity comment 9 years, 4 months ago
Lennie is an inspiration, right? Coup: from one nurse to another, I would love to see you become one of our regulars in the community; we would love to be a safe haven for you. I am proud to hear that you are working on your DNP. (jealous too) Nursing research on effective pain care—especially around integrative techniques and wellness is…[Read more]
-
Micke Brown, BSN, RN wrote a new post 9 years, 5 months ago
 Mid November 2014, I received a Maryland State Health Alert from our Secretary of Health & Mental Hygiene, Joshua M. Sharfstein, MD titled, Prescribe Naloxone and Save Lives: An Alert for Maryland Clinicians. The […]
Mid November 2014, I received a Maryland State Health Alert from our Secretary of Health & Mental Hygiene, Joshua M. Sharfstein, MD titled, Prescribe Naloxone and Save Lives: An Alert for Maryland Clinicians. The […]-

This is a very important blog for all people living with pain who are prescribed opioids. A couple months ago I attended a pain event where the speaker demonstrated how easy and quickly this medication can be administered. He spoke about how you can get an empty injector so you and your family or friends can practice the correct way to administer. So there is no guessing if the need should arise.
To answer your question this gives me comfort and does not cause alarm because I do not use illegal drugs or abuse pain medications. Having this in the house would give me comfort knowing that in the event something did happen it was there.
Some medications interact with heat and can cause the medication to be absorbed too quickly and can cause overdose. I am sure there are many opioids that have interactions like this and even though we try very hard to be very careful and do exactly what we need to do to stay safe, things can and do happen.
The FAQ you provided is also a wonderful tool.
I will be talking to my healthcare provider about this and hope that all people living with pain has the same conversation with their healthcare providers.
-
I live in NY and work in healthcare , police near me now carry narcan as overdoses happen often and they can quickly help before ambulance arrives. I like the fact that the state of yours is proactive in prevention – good for them!
-
-
Micke Brown, BSN, RN wrote a new post 9 years, 5 months ago
 Every major holiday, my second cousin opens his home to family. I, along with my brother, started joining them a few years ago following the death of my father. This new ritual became a way for me to renew my […]
Every major holiday, my second cousin opens his home to family. I, along with my brother, started joining them a few years ago following the death of my father. This new ritual became a way for me to renew my […] -
Micke Brown, BSN, RN wrote a new post 9 years, 5 months ago
 Feeling Your Best During Holiday Feasting
Feeling Your Best During Holiday Feasting
Warning! The Winter Holiday Season is Upon Us: Thanksgiving, Epiphany (Three Kings Day), Koliada, Winter Solstice, Kwanzaa, Hanukkah, Jól (Jule Eve), Christmas, Boxing […]-

I’m already failing at #s 5 and 6! I ate a ton of stuffing (my favorite) and have not recovered from it yet.
-
We have two meals. On Thanksgiving day we go to my parents and my siblings along with their families are there. Mom always makes the stuffing and it is my favorite food of the holiday also.
Our 2nd meal is here at our house usually a day or two after the official holiday.
I prepare a 25 pound turkey, deviled eggs, sweet potatoes, green beans, homemade dinner rolls, gravy, little beef franks, baked beans, stuffing and we must not forget the mashed taters for the grandkids. My children and their families come and we spend the day together.While it is a lot of work, I have found over the years that by planning for most things to be prepared in the oven, that helps keep my pain levels down.
-
-
Micke Brown, BSN, RN wrote a new post 9 years, 6 months ago
 A few weeks back, I was asked to moderate a phone support group for a kindred consumer pain organization. The topic was pacing.
A few weeks back, I was asked to moderate a phone support group for a kindred consumer pain organization. The topic was pacing.As I finished the introduction of the how’s and why’s, I listened carefully to the […]
-
Micke Brown, BSN, RN wrote a new post 9 years, 7 months ago
 I find this topic of conversation comes up a lot, especially for those who live with pain. Sleep. Will I find a comfortable position? Will I fall asleep tonight? Will I be able to sleep in my bed or will I resort […]
I find this topic of conversation comes up a lot, especially for those who live with pain. Sleep. Will I find a comfortable position? Will I fall asleep tonight? Will I be able to sleep in my bed or will I resort […]-
For me it is always the fetal position and I have to lay on my left side due to the pain in my back and neck. I don’t change positions in my sleep like some folks are able to do. I can fall to sleep easily but each night it is the same routine. Go to sleep, wake up within 2 hours. Go back to sleep (if it is a good night) and wake up within an hour or so. This goes on all night, sleep a little, wake up for a while, sleep a little, wake up. The really bad nights are the one’s I dread. Those are the nights where the pain does not allow me to sleep longer than a 1/2 hour or so and I lay there wide awake for hours at a time.
-

Me I sleep on my Left side in a pretty tight fetal position. I roll over onto Right side and onto back frequently during the night due to pain that wakes me up. A good night is to fall asleep in one position and wake up 5-6 hours later in same position. that is when I say “thank you God for a good night!” I also deal with restless leg syndrome. Some night no problem, legs are relaxed and allow me to sleep. But other nights about 6 or more nights per month – I can not get them to cooperate…they are moving all night and I find that sleep is not going to happen so that is when I get some good movies out and just vicariously sail off into another life.
In the past year I have had a real problem with sleep cycle due to changes in pain characteristics and also pain intensity. there were weeks that I had but 2-3 hours sleep per night. But I now have a sleep medication and pain meds that help to make night time something to look forward to and not dread.
Turning down the lights early in the evening helps with my sleep hygiene. Doing a Gratitude journal before bed is also helpful. and a note pad near the bed helps when my mind starts racing…I sit up get the pad, write everything down that is pouring out of my brain…then I can settle down and sleep. it is on paper…sometimes I read it in the morning but mostly I ignore it.
My favorite pillow is a contour memory foam pillow. since getting hooked on that about 10 years ago I no longer wake up with neck aches. I could not afford a memory foam mattress so I bought a 3 inch memory foam topper and I love it. Like sleeping in a cloud.
Noki4, sleepless nights are the pits. Glad I do not have them too frequently.
And Naps are my favorite thing in all the world. do not get them often but there is nothing like laying down in the middle of the day and catching an hour nap!! My motto…”when all else fails, take a nap”
-
-
Micke Brown, BSN, RN posted a new activity comment 9 years, 7 months ago
Now, how do we stop this discrimination?
-
Micke, as frustrating as it is we need to continue to stand up and shout. This past 4 months I have received 4 calls (3 in the past 2 weeks) from people in pain in WA state who need help finding resources. They find me through the Seattle times article…they write to Elin and then she refers to me. we are now banding together to approach the…[Read more]
-
-
Micke Brown, BSN, RN wrote a new post 9 years, 8 months ago
 I had an interesting conversation the other day with a journalist. No kidding! I spent about 30 minutes on the phone discussing the recent upscheduling of hydrocodone-containing combination products (HCCP). Here are some of the most common of the 65 brand names and generic medicines affected:
I had an interesting conversation the other day with a journalist. No kidding! I spent about 30 minutes on the phone discussing the recent upscheduling of hydrocodone-containing combination products (HCCP). Here are some of the most common of the 65 brand names and generic medicines affected:Vicodin, Vicodin ES, Vicodin HP
Lortab, Lorcet, Lorcet Plus
Norco
Zydone
Vicoprofen
Hydrocodone and one of the following:Aspirin (also called ASA)
Acetaminophen (also called APAP)
IbuprofenCough medicines that contains hydrocodone
He was concerned as his grandmother has been prescribed one of these preparations for her pain and wanted to understand how the change could affect her. Great grandson, right? I thought so. So, I tried to explain both sides of the issue that have been in play for several years now. He produced a nicely balanced article in my opinion. I do hope that sharing my impressions with him may have contributed. See what you think.
As I shared this news with my colleagues at TPC, I was reminded that not everyone may be up to date on the changes that have recently occurred. So, if you have not been following the recent turn of events, I will try to summarize it:
On August 22, 2014, the US Drug Enforcement Administration (DEA) issued its final rule moving hydrocodone-containing combination products (HCCP) from Schedule III to Schedule II under the federal Controlled Substances Act. The DEA’s rule will become effective on October 6, 2014.
Schedule II drugs, substances, or chemicals are defined as drugs with a high potential for abuse, less abuse potential than Schedule I drugs, with use potentially leading to severe psychological or physical dependence. These drugs are also considered dangerous.
Some examples of other Schedule II drugs are: cocaine, methamphetamine, methadone, hydromorphone (Dilaudid), meperidine (Demerol), oxycodone (OxyContin), fentanyl, Dexedrine, Adderall, and Ritalin
For other Schedules, see DEA Drug Scheduling.Those of you who have an old HCCP prescription with remaining refills will likely experience difficulty trying to get them refilled, beginning October 6, 2014.
A new prescription will be required. Why? Schedule II medications cannot be refilled.Pharmacies will be required to deny the request to fill an old prescription even if refills are indicated.
They should direct you to contact your prescriber if you do not have a new prescription.
This could cause a delay in your ability to obtain a new prescriptions and having it filled before you run out of medication. Plan ahead. Do not put yourself at risk for the onset of opioid withdrawal by running out.Your prescriber will need to use his/her own judgment on whether to require an office visit in order to obtain a new prescription or just pick it up at the front desk; office visits are not required by law, as long as the prescriber is certain that the prescription is being issued for a legitimate medical purpose, in the usual course of professional practice.
Refills can no longer be called in to the pharmacy either, EXCEPT in emergency situations, as with other Schedule II controlled substances.“In an emergency, a practitioner may call-in a prescription for a Schedule II controlled substance by telephone to the pharmacy, and the pharmacist may dispense the prescription provided that the quantity prescribed and dispensed is limited to the amount adequate to treat the patient during the emergency period.
The prescribing practitioner must provide a written and signed prescription to the pharmacist within seven days. Further, the pharmacist must notify DEA if the prescription is not received.”Some pharmacies may be reluctant to accept these emergency prescriptions because of the requirement for a follow-up written prescription. If your prescriber is unable to find a pharmacy to accept a phoned-in emergency prescription for a Schedule II medication, he/she will either need to:
Arrange for you to be seen by a prescriber in a clinic or emergency room;
Phone in a prescription for a Schedule III (e.g., codeine + acetaminophen) or Schedule IV (e.g., tramadol) opioid analgesic; or
Phone in a prescription for a non-controlled pain reliever (e.g., an NSAID).For those of you who have been given a HCCP prescription with refills in the past, the DEA does provide an option that a supply can be provided for up to 90 days. Following is the section from the DEA Practitioner’s Manual describing a Schedule II “prescription series”:
“…[A]n individual practitioner may issue multiple prescriptions authorizing the patient to receive a total of up to a 90-day supply of a schedule II controlled substance provided the following conditions are met:
Each separate prescription is issued for a legitimate medical purpose by an individual practitioner acting in the usual course of professional practice.
The individual practitioner provides written instructions on each prescription (other than the first prescription, if the prescribing practitioner intends for that prescription to be filled immediately) indicating the earliest date on which a pharmacy may fill each prescription—this is known as the “Do Not Fill Until” instructions written on a prescription.
The individual practitioner concludes that providing the patient with multiple prescriptions in this manner does not create an undue risk of diversion or abuse.
The issuance of multiple prescriptions is permissible under applicable state laws.
The individual practitioner complies fully with all other applicable requirements under the Controlled Substances Act and Code of Federal Regulations, as well as any additional requirements under state law.”Basically, this provision allows a prescriber to issue prescriptions totaling a 90-day supply in a variety of ways: 3 prescriptions each with a 30 day supply; 6 prescriptions each with a 15 day supply; or as many as 90 prescriptions with a one-day supply, if needed.
The ability to do this has been poorly understood by many prescribers, therefore, not frequently used. It is anticipated that with the need to replace a very large number of HCCP refills (about 26 million per year nationwide), the use of this practice just might become more common.
[I would be remiss if I did not give a shout out to one of my favorite pain advocates. Thank-you, Bob Twillman of the American Academy for Pain Management, for making this information so easy to share].
Before closing, I must also share another bit of news that some may have missed. Tramadol (Ultram, Ultracet) was placed in the Schedule IV class by the DEA effective on August 18th, 2014. It joins the ranks with other medications like: Xanax, Soma, Valium, Ativan, Talwin, Ambien.
Please let me know if you experience any hurdles with these changes in regulations and lessons learned so others may benefit.
-
Micke, great info. thanks
-
-
Micke Brown, BSN, RN posted a new activity comment 9 years, 8 months ago
Kudos for your frankness, Teresa! This is one blog that all must share and encourage comments from the many who live with pain everyday. You are so right—Enough is enough and together we must scream, holler and shout. If not, we are to blame that pain care does not improve and this terrible state of affairs does not return to sanity and humane discourse.
-
Micke Brown, BSN, RN wrote a new post 9 years, 9 months ago
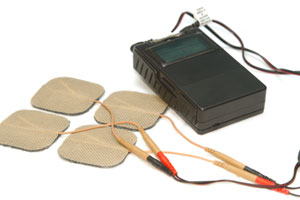 A few weeks back, I was talking with a friend who lives with pain. What she told me I had heard before yet it continues to stay on my mind. Her physician prescribed a TENS unit as another way to treat her back […]
A few weeks back, I was talking with a friend who lives with pain. What she told me I had heard before yet it continues to stay on my mind. Her physician prescribed a TENS unit as another way to treat her back […] -
Micke Brown, BSN, RN wrote a new post 9 years, 9 months ago
 I remember when I was in grammar school, being asked to write about how I spent my summer vacation. As an adult, I have been remiss and did not plan summer vacations on a regular basis, if at all. This year was […]
I remember when I was in grammar school, being asked to write about how I spent my summer vacation. As an adult, I have been remiss and did not plan summer vacations on a regular basis, if at all. This year was […] -
Micke Brown, BSN, RN replied to the topic Painiac Shuffle, Move & More in the forum Wellness Issues 9 years, 10 months ago
I have to share a success story. I was traveling with my 81 year old cousin to a family reunion over this past weekend. He has rheumatoid arthritis and becoming less steady on his feet. He also told me that he had pulled his hamstring several times over the recent weeks. However, he insists on walking whenever he can as he fears that one he stops,…[Read more]
-
Micke Brown, BSN, RN replied to the topic Painiac Shuffle, Move & More in the forum Wellness Issues 9 years, 10 months ago
I am thinking that walking is the easiest for most of us to do. You can do it anytime, anywhere, at your own pace, only need a good pair of tennis shoes and you are off. If you need a walking stick, cane or walker—decorate it and strut your stuff!! Walk your dog, grab your partner, a good friend or a neighbor–then go. You may only walk out to…[Read more]
-
Micke Brown, BSN, RN commented on the post, Relationships: Are You in Ones of Comfort or Chaos? 9 years, 10 months ago
I found myself thinking back on similar relationships in my past too. “What does not kill us makes us stronger” comes to mind. I am happy to hear that this information resonates with to you and hopefully others. […]
-
Micke Brown, BSN, RN wrote a new post 9 years, 10 months ago
 While attending a public event recently, I found myself drawn to a particular display booth of an organization that helps others who have experienced the violence of abuse. As I browsed through their brochures, […]
While attending a public event recently, I found myself drawn to a particular display booth of an organization that helps others who have experienced the violence of abuse. As I browsed through their brochures, […] -
Micke Brown, BSN, RN replied to the topic Medication interactions and warnings in the forum Treatment Options for Pain 9 years, 10 months ago
One BIG concern that I have and have been following is the combination of opioid pain medications and benzodiazepines (like valium, xanax, klonopin, ativan and others) used as sleep agents or to lower anxiety. A report just came out from the Maryland Dept of Health about this and its role in prescription medication overdose. The warning is this:…[Read more]
- Load More
I plan to got see this one at the movie theater!
I look forward to seeing this movie.